Robotic Surgery Strengthens Abdominal Wall, Prevents Hernia Recurrence
November 2, 2020Categories: Feature
Robotic technology has given way to an array of innovative surgical techniques for the treatment of abdominal wall hernias. Two new minimally invasive techniques -- extended-view totally extraperitoneal repair and eTEP repair with transversus abdominis release -- aid in the treatment of umbilical, ventral, incisional and recurrent hernias.
Extended View
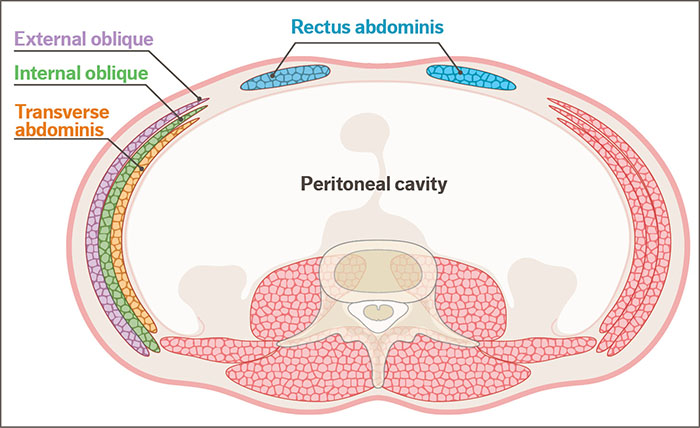
“With eTEP, we can do large, complex hernia repairs by working between layers of the abdominal wall without entering the peritoneal cavity, where patients who have had numerous procedures may have a great deal of scar tissue, which complicates hernia surgery,” said Joshua M. Mourot, MD, FACS, a general surgeon with Meritas Health Comprehensive Surgery. “By rebuilding the abdominal wall, we restore normal anatomy and function and reinforce the repair with mesh to reduce hernia recurrence.”
During an eTEP procedure, Dr. Mourot reduces the hernia and simultaneously releases the muscular attachments that lead to tension on the repair and possible hernia recurrence. Additionally, by performing the repair outside the peritoneal cavity, the mesh used for strengthening the repair does not come in contact with abdominal contents, such as the small intestine and colon. This potentially reduces the risk for mesh-related complications, including an intestinal fistula or bowel obstruction.
For larger hernias that may require further relief of tension to completely close, Dr. Mourot may release the transversus abdominis muscle. The size and shape of the hernia and the compliance/tension of a patient’s abdominal wall determines whether he performs an eTEP or eTEP with TAR.
An eTEP repair takes about 90 minutes to two hours, and patients typically go home the same day. An eTEP repair with TAR is approximately two to four hours, and patients typically stay overnight.
Recurrence Prevention
“With very large hernias, significant lateral force from the abdominal wall musculature may lead to hernia recurrence. If a hernia is repaired under high tension, these forces may lead to recurrence even with the slightest patient cough,” Dr. Mourot noted. “By releasing the rectus muscles in eTEP and additionally releasing the transversus abdominis in eTEP with TAR, that tension is offloaded.”
He added that obesity, smoking and heavy weight-lifting immediately following surgery also lead to hernia recurrence.
“We possess an armamentarium of techniques to fix hernias in a minimally invasive fashion with the robotic platform, and we’re making great strides,” Dr. Mourot said. “Improved vision and dexterity in a small space, as is the case with eTEP, allows us to repair large, complex hernias in a minimally invasive way and gets patients back on their feet more quickly.”

Joshua M. Mourot, MD, FACS
Dr. Mourot earned his medical degree from the University of Texas Medical Branch and completed his residency in general surgery and a fellowship in advanced minimally invasive surgery at the University of Washington.